

Background: To better understand the clinical practice in Germany with respect to the rapidly evolving treatment landscape, we aim to describe the characteristics and treatment patterns of patients (pts) with relapsed/refractory multiple myeloma (RRMM) in Germany.
Methods: In a national retrospective medical chart review including consecutive pts treated for RRMM in participating hospitals/centers and practices across Germany between Oct 2017 and Jun 2018, the following data were extracted from Oct 2019 to Feb 2020: pt demographics, disease characteristics, treatment history at MM diagnosis and at initiation of RRMM therapy, and distance to care. Physician's assessment of response to therapy and minimal residual disease (MRD) testing were also collected. Because this analysis was not powered to compare between regimens or lines of therapies, results are purely descriptive.
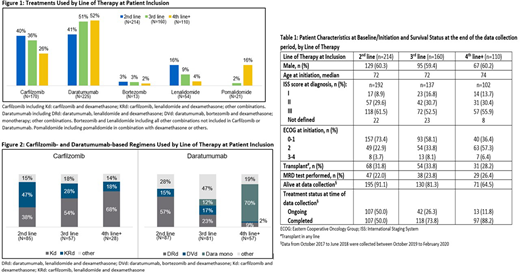
Results: Physicians from 47 participating centers extracted 484 pt charts, that included 214 pts (44%) in 2nd line of therapy (2L), 160 (33%) in 3rd line (3L) and 110 (23%) in 4th line and beyond (4L+) (Figure 1). Half of the participating centers were office-based (52%) and 40% were hospitals. Results are summarized in Table 1 and regimens described by line of therapy in Figure 2:
Among the 2L subgroup (N=214), median age was 72 years and the majority (73%) of pts had an ECOG status of 0-1 at 2L initiation. About one-third (31%) of pts had had a transplant. Carfilzomib (CFZ) or daratumumab (Dara)-based regimens were mainly used in 2L pts (40% and 41%, respectively). Among the 87 Dara pts, the triplet regimen Dara, lenalidomide (LEN) and dexamethasone (DRd) was used in more pts (58%) than the triplet with Dara, bortezomib (BTZ) and dexamethasone (DVd, 15%). Among the 85 CFZ pts, nearly half (47%) received the triplet regimen CFZ, LEN and dexamethasone (KRd) and 38% of CFZ pts received the doublet of CFZ and dexamethasone (Kd). Among the remaining 42 pts in 2L, other LEN use was described in 35 pts and BTZ in 7 pts. For 107 pts who completed 2L, median treatment duration was 8 months (9 months for CFZ pts; 8.5 months for Dara pts; 6 months for LEN pts). Where response was available (n=191/214), a complete response (CR) or very good partial response (VGPR) was achieved by 64% of pts, including 73% of Dara pts (n=53/73), 62% of CFZ pts (n=48/78), and 53% of LEN pts (n=18/34). 149 ptssteoprotective drugs at 2L initiation, mainly intravenous zoledronate (ZA, 44%) and subcuteaneous denosumab (Dmab, 42%).
In the 3L subgroup (N=160), median age was 72 years. Over half (58%) of pts had an ECOG status of 0-1 at 3L initiation. Most 3L pts received Dara (51%, n=81) or CFZ (35%, n=57), and a further 9% (n=15) of 3L pts received other LEN combinations. In 3L, CFZ was more often used as a doublet (54% Kd vs. 28% KRd); Dara was mainly given in triplet regimens (23% DRd, 17% DVd vs. 12% Dara mono). For 118 pts who had completed 3L at time of data extraction, median treatment duration was 10 months (10 months for both CFZ and Dara pts, 7 months for LEN pts). Where response was available (n=139), CR/VGPR was achieved by 55% of pts in 3L, including 64% of Dara pts (n=46/72) and 41% of CFZ pts (n=20/49). Osteoprotective drugs (51% Dmab, 36% ZA) at 3L initiation were given in 69% (n=111) of pts.
In the 4L+ subgroup (N=110), median age was 74 years. A high percentage (64%) of pts had an ECOG status ≥2 at 4L initiation. Over half (52%, n=57) received Dara, mostly as monotherapy (70% Dara; 9% DRd, 2% DVd), followed by CFZ in 26% (n=28) and pomalidomide (POM) in 16% (n=18) of pts in 4L+. For 97 pts who completed 4L at time of data extraction, median treatment duration was 8 months (9 months for both CFZ and Dara pts, 7 months for POM pts). Where response was available (n=106), 39% of pts achieved a CR/VGPR, including 46% of Dara pts (n=25/55) and 36% of CFZ pts (n=10/28). At 4L initiation, 66% (n=72) of pts were receiving osteoprotective drugs (51% Dmab, 40% ZA).
Conclusion: This chart review indicates that pts with RRMM who underwent a MM therapy between Oct 2017 and Jun 2018 in routine practice across Germany, mostly received combination regimens with novel agents irrespective of the line of therapy. Lenalidomide is still often combined with novel agents. Patterns of treatment regimens differed by line of therapy and are adapted as disease progresses and ECOG status increases.
Steinmetz:Amgen; BMS, Celgene, Novartis; Janssen-Cilag; Omnicare, Vifor: Speakers Bureau; Amgen: Membership on an entity's Board of Directors or advisory committees; Alexion, Amgen, Bayer, BMS, Boehringer, Celgene, Janssen-Cilag, Novartis, Omnicare, Sanofi, Takeda: Other: TRAVEL, ACCOMMODATIONS, EXPENSES; DGHO, ESMO, DGPM, BNHO, NIONo: Other: Memberships; Alexion, Accord Healthcare, Amgen; Ariad, Bluebird Bio, BMS, Boehringer, Celgene, Hexal-Sandoz, Novartis; Janssen-Cilag; Omnicare, Oncopeptides, Otsuka, Pfizer, Sanofi, Shire, TAD, Takeda, Vifor: Consultancy; Accord Healthcare, Amgen, Celgene, Novartis, Vifor: Research Funding. Singh:Amgen Ltd, UK: Current Employment. Milce:Amgen: Research Funding; Kantar Health, France: Current Employment. Haidar:Kantar Health, France: Current Employment; Amgen: Research Funding. Rieth:Amgen GmbH, Germany: Current Employment; Amgen: Current equity holder in private company. Lebioda:Amgen GmbH, Germany: Current Employment; Amgen: Current equity holder in private company.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal